
Every 4 years, we travel to a new city and get to watch the world’s most dedicated and physically talented athletes compete in a wide range of sports. While the olympics are steep in tradition stemming all the way back to 1896 in Athens, Greece, today we get to see modern athletes and its draws a crowd unlike any other. From London 2012, to Rio 2016, to Tokyo 2020, we get to travel some of the world’s finest cities, take in their food and culture, and enjoy the company of athletes as the olympics take place. While Tokyo is sure to deliver all of those things, one thing to be aware of is the risk of contracting illnesses or diseases in a crowded area during a specific high risk period. Stay tuned for my next post on the “new polio” and precautions to avoid this highly contagious disease.
Hand, Foot and Mouth Disease
Just like flu season in the United States, Hand, Foot and Mouth disease is an epidemic observed annually in the Asia-Pacific region for the last two decades.
What is it?
Hand, Foot and Mouth Disease (HFMD) is an infectious viral illness that mostly affects children less than 5 years old (90%), but can also occur in older children and adults. HFMD is caused by a group of enteroviruses, most commonly the Coxsackievirus (CA16) and Enterovirus 71 (EV71). In contrast to CA16 cases, which are often mild and self-limiting, those infected by EV71 have a higher risk of developing severe complications.
Symptoms:
HFMD commonly starts with
- Fever
- Sore throat
- Malaise (unwell feeling)
- Reduced appetite
1 or 2 days later,
- Painful oral ulcers (Herpangina) typically in back of the mouth
- Rash/blisters on palms/soles of the feet (non-itchy)
- Less commonly appear on knees, elbows, buttocks, or genital area

Rare, life-threatening cases of HFMD can infect the central nervous system causing viral meningitis or encephalitis (<1%). Symptoms include/not limited to:
- Vomiting
- Lethargy
- Agitation
- Irritability
- Tremors
- Myoclonic jerk movements
*Not everyone may get all symptoms. Infected adults may show NO symptoms, but may be transmissible*
Transmission:
- Direct contact with someone infected, touching infected blister fluid or stool after changing a diaper
- Infected person sneezing/coughing around you
- Touching infected surfaces (toys or doorknobs) and then touching your eyes, nose, or mouth
Treatment:
HFMD is a self-limiting illness with majority recovering spontaneously. Treatment is aimed to improve symptoms. Mild cases resolve within 7-10 days. Those infected should not return to day-care, school, or work until sores have healed.
- Acetaminophen or ibuprofen for pain and fever, throat sprays to numb pain
- Children may experience significant throat discomfort which can lead to dehydration requiring IV fluids
What you should know:
Historically, the occurrence of HFMD changed in the 1990’s from its previous sporadic pattern. Since 1997, medium- to large-scale epidemics have been observed annually in the Asia-Pacific region, with most cases associated with EV71. Every three years a rise in the number of cases exists and is attributed to a three year cyclical component of EV71. As vaccinations have almost eradicated the Poliovirus, EV71 has now become the most frequent enterovirus to cause severe CNS infections and has emerged as the “new polio”. Although serious complications are rare, some Japanese epidemics have had unusual high numbers of fatalities, generating public fear and anxiety.
Disease surveillance has shown consistent seasonal trends, with peak HFMD diagnosis during weeks 31 and 32.
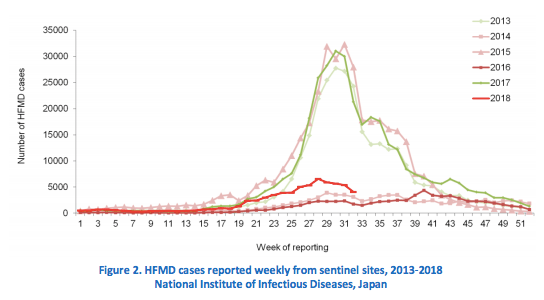
Weeks 31-32 of 2020 fall between July 27th and August 9th.
Summer Olympics of 2020 begin July 24th and end August 9th.
Prevention:
- Avoid contact with those infected
- Cover yourself when you cough or sneeze
- Avoid touching eyes, nose, mouth with unwashed hands
- Wash your hands often with soap and water for at least 20 seconds
- Disinfect frequently touched surfaces and soiled items
Resources:
References:
Biggs, H.M. (2019 June 24). Hand, Foot, & Mouth Disease. Travelers’ Health: Travel-Related Infectious Diseases. Retrieved from https://wwwnc.cdc.gov/travel/yellowbook/2020/travel-related-infectious-diseases/hand-foot-and-mouth-disease
Chang, L.-Y., Tsao, K.-C., Hsia, S.-H., Shih, S.-R., Huang, C.-G., Chan, W.-K., … Lin, T.-Y. (2004). Transmission and clinical features of enterovirus 71 infections in household contacts in Taiwan. JAMA, 291(2), 222–227. Retrieved from http://search.ebscohost.com.ezproxy.neu.edu/login.aspx?direct=true&db=cmedm&AN=14722149&site=ehost-live&scope=site
Gonzalez, G., Carr, M. J., Kobayashi, M., Hanaoka, N., & Fujimoto, T. (2019). Enterovirus-Associated Hand-Foot and Mouth Disease and Neurological Complications in Japan and the Rest of the World. International Journal Of Molecular Sciences, 20(20). https://doi-org.ezproxy.neu.edu/10.3390/ijms20205201
Tang, J.-H., Chan, T.-C., Shigematsu, M., & Hwang, J.-S. (2015). Latitude-based approach for detecting aberrations of hand, foot, and mouth disease epidemics. BMC Medical Informatics And Decision Making, 15, 113. https://doi-org.ezproxy.neu.edu/10.1186/s12911-015-0236-5
World Health Organization, Regional Office for the Western Pacific, (2018). Hand, Foot and Mouth Disease. Manila: WHO Regional Office for the Western Pacific. Retrieved from https://iris.wpro.who.int/handle/10665.1/14191
